An internet resource developed by
Christopher D. Green
York University, Toronto, Ontario
(Return to Classics index)
by Mr. Paul Broca (1861)
Surgeon of the Bicêtre Hosptial
First published in Bulletin de la Société Anatomique, 6, 330-357.
Translation by Christopher D. Green
© Christopher D. Green 2000
All rights reserved
(go to French original)
[Translator's Note: I have made an explicit attempt to keep this translation as literal as possible, which accounts for some of its clumsiness in English. For instance, I have rendered "langage articulé" as "articulated language" throughout, rather than as the perhaps more felicitous "spoken language," in order to maintain the technical style, and to distinguish it from the more colloquial "langage parlé." I have also refrained from using the seemingly more felicitous, but less precise, "articulate language." In addition, I have often used "ill people" for "malades" rather than "patients," especially in the first half of the article, because it emphasizes their condition rather than their relationship to the physician. I have also tried to retain the archaic vocabulary as much as possible. Special thanks to Classics Editorial Assistant, Daniel Denis, whose recommendations improved the translation immeasurably. -cdg-]
The paper and remarks that I am presenting to the Anatomical Society comes to the defense of the ideas professed by Mr. Bouillaud concerning the seat of the faculty of language. This question, both physiological and pathological, merits more attention than most doctors have accorded it up to now, and the matter is delicate enough, the subject obscure enough, and complex enough, that it seems useful to begin with some remarks relating the facts that I have observed.
I.
We know that the phrenological school placed at the front part of the brain, in one of the convolutions that lie on the orbital arch, the seat of the faculty of language. This opinion, which had been accepted, like so many others, without sufficient evidence, and which besides rested only on a very imperfect analysis of language phenomena, would have without doubt disappeared with the rest of the system, if Mr. Bouillaud had not saved it from foundering by making some important modifications to it, and by surrounding it with a parade of evidence borrowed above all from pathology. Without considering language as a simple faculty dependent on a single cerebral organ, and without looking to hem into an area of a few millimeters the location of this organ, as had been done by Gall's school, this professor was led by the analysis of a great number of clinical facts, followed by autopsies, to concede that certain lesions of the hemispheres abolish speech without destroying intelligence, and that the lesions always [p. 331] have their seat in the frontal lobes of the brain. He concluded that somewhere in these lobes, one or several convolutions holds under their dependence one of the elements essential to the complex phenomenon of speech, and thus, less restricted than in Gall's school, placed in the frontal lobes, without specifying further, the seat of the faculty of articulated language, which must not be confused with the general faculty of language.
There are, in effect, several species of language. Any system of signs permitting the expression of ideas in a manner more or less intelligible, more or less complete, more or less rapid, is a language in the most general sense of the word: thus speech, mimicry, typing [dactylologie], picture writing [l'écriture figurative], phonetic writing, etc., are all species of language.
There is a general faculty of language that presides over all these modes of the expression of thought, and it may be defined: the faculty of establishing a constant relation between an idea and a sign, whether this sign be a sound, a gesture, a figure, or any other trace. Moreover, each species of language necessitates the play of certain organs of emission and reception. The organs of reception are sometimes the ear, sometimes sight, sometimes even touch. As for the organs of emission, they are put in play by the voluntary muscles, like those of the larynx, or the tongue, of the soft palate [voile du palais], of the face, the upper limbs, etc. All regular language supposes therefore the integrity, (1) of a certain number of muscles, of the motor nerves that serve them, and the part of the central nervous system from which these nerves arise; (2) of a certain external sensory apparatus, of the sensory nerve that departs from these, and of the part of the central nervous system to which this nerve connects; (3) finally, the part of the brain that holds under its dependence the general faculty of language, such as we have come to define it.
The absence or abolition of this last faculty renders impossible all species of language. Congenital or accidental lesions of the organs of reception and the organs of emission can deprive us of the particular species of language that these organs contribute; but if the general language faculty persists in us with a sufficient degree of intelligence, we can still compensate with another species of language for those we have lost. [p. 332]
The pathological causes that deprive us of a medium of communication ordinarily make us lose only half of it, because it is quite rare that the organs of emission and the organs of reception would be affected at the same time. For example, the adult who becomes deaf continues to express himself through speech, but for him to transmit an idea he uses a different language, such as gesture or writing. The inverse takes place when paralysis strikes the speech muscles; the ill person to whom we address ourselves in articulated language, responds to us then in another language. It is in this way that diverse systems of communication can be mutually compensatory.
This is only elementary physiology; but pathology permits us to push the analysis further on to that which concerns articulated language, which is the most important and probably the most complex of all.
There are cases where the general language faculty persists unaltered, where the auditory apparatus is intact, where all the muscles, not even excepting those of the voice and those of articulation, obey the will, and yet where a cerebral lesion abolishes articulated language. This abolition of speech, in individuals who are neither paralyzed nor idiots, constitutes a symptom so singular that it seems to me useful to designate it with a special name. I will give it, therefore, the name of aphemia (a deprive; jhmi, I speak, I pronounce); it is only the faculty of articulating words that these patients lack. They hear and comprehend all that one says to them; they all have their intelligence; they emit vocal sounds with ease; they execute with their tongue and their lips movements much more extensive and energetic than those required for the articulation of sounds, and yet the perfectly sensible response that they would want to make is reduced to a very small number of articulated sounds, always the same and always performed in the same manner; their vocabulary, if can call it that, is composed of a short series of syllables, sometimes of a monosyllable that expresses everything, or rather that expresses nothing, for this unique word is most often a stranger to all vocabularies. Certain ill people have not even a vestige of articulate language; they make vain efforts without pronouncing a single syllable. Others have, in some sense, two degrees of articulation. In [p. 333] ordinary circumstances, they invariably pronounce their word of choice [prédilection]; but, when they have an angry outburst, they become able to articulate a second word, most often a coarse swearword, with which they were probably familiar before their sickness, then they stop after the latter effort. Mr. Auburtin has observed a patient who is still alive and who does not need to be excited to utter a stereotyped curse. All his responses start with a bizarre word of six syllables and invariably end with this supreme invocation: Sacred name of G...
Those who have for the first time studied these strange happenings have been able to believe, due to an [in-?]sufficient analysis, that the faculty of language, in similar cases, was abolished; but it obviously persists in its entirety, since these ill people perfectly comprehend articulated language and written language; since these who do not know how or are not able to write have enough intelligence (and it is mistaken in many similar cases) to find the means to communicate their thought, and since finally those who are literate, and who have the free use of their hands, clearly put their ideas on paper. They know therefore the sense and the value of words, in auditory form just as in graphic form. Articulated language that they could once speak is always familiar to them, but they cannot execute the series of methodical and coordinated movements that correspond to the searched-for syllable. This which has died in them [péri en eux], it is not therefore the faculty of language, it is not the memory for words, nor is it the action of the nerves and muscles corresponding to phonation [phonation] and to articulation, it is something else, it is a faculty particularly considered by Mr. Bouillaud as the faculty that coordinates the proper movements of articulated language, or more simply as the faculty of articulated language, since without it there is no articulation possible.
The nature of this faculty and the place that it must be assigned in the cerebral hierarchy can give rise to some hesitation. Is it only a species of memory, and the individuals who have lost it have lost only, not the memory of words, but memory for the procedure that must be followed to articulate words? Have they come to this by a condition comparable to that of a young child who already understands the language of those around him, who is sensitive to blame and praise, who points out with his fingers all the [p. 334] objects that he can name, who has acquired a crowd [foule] of simple ideas, and who, to express these, can do no more than stammer out a single syllable? Little by little, after innumerable efforts, he succeeds in articulating a few new syllables. Yet still he arrives so often at a mistake, saying, for example, papa when he wanted say mama, because at the moment of pronunciation of the latter word he no longer remembers the position that must be given to his tongue and to his lips. Soon he knows quite well the mechanism of some simple and easy syllables so that he can pronounce them at every attempt without error and without hesitation; but he hesitates and again makes mistakes on more complicated and more difficult syllables, and when finally he possesses much practical experience with [la practique de] many monosyllables, he needs to acquire new experience to learn to pronounce rapidly [passer tout à coup] one syllable after another, and to pronounce, in the place of the doubled monosyllables that constituted his first vocabulary, words composed of two or three different syllables. These gradual perfections of articulated language in children are due to the development of a particular species of memory that is not the memory for words, but that of the movements necessary to articulate words. And this particular memory is not related [en rapport] to other kinds of memory nor to the rest of intelligence. I knew a child of three years whose intelligence and will was above that of his age, who had a well-formed tongue, and who still did not know how to talk. I know another very intelligent child who, at the age of twenty-one months, perfectly understands two languages, who, as a consequence, possesses the highest degree of memory for words, and who up to this point, is not able to rise above the level of pronouncing monosyllables.
If adults who lose speech have only forgotten the art of articulation, if they have simply reverted [revenus] to the condition where they were before having learned to pronounce words, we must place [ranger] the faculty of which the illness has deprived them into the order of intellectual faculties. This hypothesis seems to me quite likely. It might be possible, however, that it is otherwise, and that aphemia is the result of a locomotor ataxia limited to the part of the central nervous apparatus that presides over movements governing the articulation of sounds. One objects, it is true, that these ill people can freely [p. 335] execute with their tongue and their lips all the movements other than those of articulation; that they can immediately move, when asked, the point of their tongue upwards, downwards, to the right, to the left, etc.; but these movements, precise as they may seem to us, are infinitely less so than the excessively delicate movements that are required for speech. In locomotor ataxia of the limbs, one observes that the patients voluntarily execute all the large movements: if one tells them to lift their hand, to open it, to close it, they do it almost always without hesitation; but when they want to execute more precise movements, to seize, for example, in a certain manner, an object of small volume, they go beyond or stay behind the goal; they do not know how to coordinate the contraction of their muscles in a manner to obtain a result of determined value, and they make mistakes much less in the direction of their movements than in the quantity of force that they have to deploy and in the order of succession of partial movements of which the grasping of objects is composed. One can therefore ask if aphemia is not one species of locomotor ataxia limited to the muscles for the articulation of sound, and, if it were so, the faculty that the ill people have lost would not be an intellectual faculty, that is to say a faculty belonging to the thinking part of the brain, it would be only a particular case of the general faculty of coordination of muscular action, a faculty that depends on the motor parts of the nerve centers.
One can therefore make at least two hypotheses about the nature of the special faculty of articulated language. In the first hypothesis, there would be a superior faculty, and aphemia would be an intellectual trouble; in the second hypothesis, it would be a faculty of a much less elevated order, and aphemia would be no more than a trouble of locomotion. Though the latter interpretation appears to me much less probable than the other, I would not yet dare to commit myself in a categorical manner if I were reduced to only the lights of clinical observation.
Whatever it might be, on the account of functional analysis, the existence of the special faculty of articulated language, such as that I have defined, cannot be placed in doubt, because a faculty that can perish alone, without those that are nearest to it being [p. 336] altered, is obviously a faculty independent of all the others, that is to say a special faculty.
If all the cerebral faculties were as distinct, as clearly circumscribed as this one, one would finally have a positive point of departure to enter upon the question so controversial as cerebral localization. It is unfortunate that this is not so, and that the greatest obstacle to progress in this part of physiology comes from the insufficiency and uncertainty of the functional analysis that must necessarily precede research on the organs related to each function.
Science is so little advanced on this point that it still has not even found its foundation, and what is in dispute today is not such-and-such phrenological system, but the very principle of localization, that is to say the prior question is knowing whether all parts of the brain that are concerned with thought have identical attributes or different attributes.
A communication of Mr. Gratiolet relevant to the cerebral and intellectual similarity of the human races, has, on several occasions, detained the Anthropological Society of Paris to examine this important question, and Mr. Auburtin, partisan of the principle of localization, has thought, with good reason, that the localization of a single faculty suffices to establish the truth of this principle; he has, therefore, sought to demonstrate, according to the doctrine of his teacher Mr. Bouillaud, that the faculty of articulated language resides in the frontal lobes of the brain.
For this, he first reviewed a series of cases in which a spontaneous cerebral event had abolished the faculty of articulated language without destroying the other cerebral faculties, and in which at autopsy a deep lesion was found in the frontal convolutions of the brain. The special nature of the symptom of aphemia did not depend on the nature of the illness, but only on its location [siège], since the lesion was sometimes a softening, sometimes apoplexy, sometimes an abscess or a tumor. To complete his demonstration, Mr. Auburtin invoked another series of cases where aphemia was the consequence of a traumatic lesion of the frontal lobes of the brain; these facts, following him, the equivalent of vivisections, and he ended by saying that to his knowledge no one has ever found the frontal lobes of the brain in a state of complete [p. 337] integrity, nor even in a state of relative integrity, at the autopsy of individuals who have lost the faculty of articulated language without losing the rest of their intelligence.
Some have opposed him with many remarkable facts relevant to individuals who had spoken right up to the last day, and yet in whom the frontal lobes of the brain had been the seat of deep spontaneous or traumatic lesions; but he responded that this proves nothing, that a lesion, even widespread, of the frontal lobes might not reach the part of the lobes where resides [siége] the faculty of articulated language, that the objection would only be valid if all the frontal convolutions had been destroyed on both sides to their full extent, that is to say up to the sulcus [sillon] of Rolando, and that, in the cases opposed to him, the destruction of the convolutions had been only partial. He therefore recognized that a lesion of the frontal lobes does not necessarily lead to a loss of speech, but he maintained that the latter is the certain sign of the former, that it permits such a diagnosis; that the diagnosis has been made many times during life, and has never been refuted [démenti] by autopsy; finally, after having cited the observation of a still-living individual who presents for many years in a most clean manner, the symptoms of aphemia, and who is actually at the hospice for Incurables, he declared that would renounce without reversion [retour] the doctrine of Mr. Bouillaud, if the autopsy of this ill person did not confirm the diagnosis of a cerebral lesion occupying exclusively or principally the frontal lobes. (see Bulletin de la Société d'anthropologie, 1. II, meeting of 4 April, 1861.)
I believe I should summarize in a few words this discussion to make salient the interest and the actuality of the observation that I am presenting today to the Anatomical Society. Without doubt, the value of facts is not limited [subordonnée] to the circumstances of the milieu in which we observe them; but the impression that they make on us depends on them in great part, and when, a few days after having heard the argument of Mr. Auburtin, I found one morning, in my care [service], a dying person who for twenty-one years had lost the faculty of articulated language, I collected with the greatest care observations from him, which seemed to come expressly to serve as a touch stone [pierre de touche] for the theory supported by my colleague. [p. 338]
Up to here, without rejecting the theory, and without ignoring as nothing the importance of the facts that are favorable to it, I had felt much hesitation in the presence of the contradictory facts that exist in science. Though a partisan of the principle of localization, I would ask myself, and I ask myself still, within what limits this principle is applicable. There is a point that appears to me to be pretty nearly established by comparative anatomy, by the anatomical and physiological parallel of the human races, and finally by the comparison of the varieties of normal individuals, abnormal or pathological men of the same race; to know that the highest cerebral faculties, those that constitute the understanding properly so-called, like judgment, reflection, the faculties of comparison and abstraction, have their seat in the frontal convolutions, while the convolutions of the temporal, parietal, and occipital lobes are involved with [affectées aux] the sentiments, the dispositions [penchants], and the passions. In other terms, there is in the mind [esprit] groups of faculties, and in the brain, groups of convolutions; and the facts acquired up to now by science permit us to accept, like I have said elsewhere, that the large regions of the mind [esprit] correspond to the large regions of the brain. It is in this sense that the principle of localization seems to me, if not [sinon] rigorously demonstrated, at least extremely probable. But to know with certainty whether each particular faculty has its own seat in a particular convolution, this is a question that seems to me all but insoluble in the current state of science.
The study of the facts relevant to the loss of the faculty of articulated language is one those that has the most chance of leading us to a positive or negative solution. The independence of this faculty is evinced by pathological observation, and though one can raise some doubts about its nature, though one can ask oneself, as has been seen above, if it is part of the intellectual functions or of the cerebral functions that are involved [en rapport] with muscular activity, it is allowable to place it, at least provisionally, in the purview of the first hypothesis, which already, at first glance, seems the most probable, and in favor of that which the pathological anatomy of aphemia establishes strong presumptions. In effect, in all the cases where up to now the autopsy has been able to be undertaken, one has found the substance of the convolutions [p. 339] profoundly altered to a notable extent; in a few subjects the lesion spread exclusively over the convolutions where it is permitted to conclude that the faculty of articulated language is one of the functions of the convoluted mass. Now, one admits generally that all the faculties we call intellectual have their seat in this part of the brain, and it seems from that strongly probable that reciprocally all the faculties that reside in the cerebral convolutions are faculties of the intellectual order.
In placing ourselves, then, in this point view, we easily recognize that the pathological anatomy of aphemia can give something more than a solution to one particular question, and that it can throw a great deal of light on the general question of cerebral localization, by furnishing to cerebral physiology a point of departure, or rather a very precious point of comparison. If it were proven, for example, that aphemia can be the result of lesions affecting indifferently in any convolution and in any cerebral lobe, one would have the right to conclude not only that the faculty of articulated language is not localized, but also that very probably the other faculties of the same order are not localized either. If it were demonstrated on the contrary that the lesions that abolish speech consistantly occupy one determinate convolution, one could hardly fail to admit that this convolution is the seat of the faculty of articulated language, and, that once the existence of a first localization was admitted, the principle of localization by convolutions would be established. Finally, between these two extreme alternatives, there is a third that could lead to a mixed doctrine. Let us suppose, in effect, that the lesions of aphemia consistently occupy the same cerebral lobe, but that, in this lobe, they do not consistently occupy the same convolution; it would result that the faculty of articulated language would have its seat in a certain region, in a certain group of convolutions, but not in a particular convolution, and it would become very probable that the cerebral faculties are localized by regions, and not by convolutions.
It is important [importe], therefore, to study with the greatest care a special question that can have doctrinal consequences so general [p. 340] and so important. It is not only a matter of looking in which regions of the brain are located [siégent] the lesions of aphemia; one must as well designate by name and by row the affected [malades] convolutions and the degree of alteration of each. This is not how we have proceeded up to now. We have confined ourselves, in the most complete observations, to saying that the lesion began and finished so many centimeters from the frontal extremity of the hemisphere, so many centimeters from the great central fissure [scissure] or from the Sylvian fissure. But that is completely insufficient, because, given these indications, meticulous as they are, the reader cannot guess which is the affected convolution. Thus, there are cases where the illness is situated in the most frontal part of the hemisphere; others where it is situated 5 or even 8 centimeters behind this point, and it seems, given this, that the seat of the lesion might be very variable; but if one imagines [songe] that the three antero-posterior convolutions of the convexity of the frontal lobe begin at the level of the sourciliary arcade and run side by side, front to back, all three flowing into the frontal transverse convolution that forms the anterior side of the sulcus [sillon] of Rolando; if one imagines that this sulcus is situated more than 4 centimeters behind the coronal suture[1], and [p. 341] that the three frontal antero-posterior convolutions occupy more than two-fifths of the total length of the brain, -- one will understand that the same convolution is able to be reached by lesions situated in points very different and very distant from each other. It is therefore, much less important to indicate the level of damage [mal] than to say which convolutions are ill.
This kind of description is without doubt less convenient than the other, for the classical anatomy treatises have not vulgarized up to now the study of cerebral convolutions that the phrenologists themselves had made the great mistake of neglecting. One is left to be dominated by the old prejudice that the cerebral convolutions have nothing fixed about them, that they are simple folds made haphazardly, comparable to the disordered bendings [flexuosités] of the intestinal loops, and what has accredited this idea, is that the secondary folds, which depend on the degree of development of the fundamental convolutions, vary not only from individual to individual, but often even within the same individual, from one hemisphere to the other. It is no less true that these fundamental convolutions are fixed and constant in all animals of the same species, and that, considered in the animal hierarchy, they behave much like perfectly distinct organs. The description and enumeration of the fundamental convolutions, of their connections and of their associations [rapports], would find no place here. One will find them in the special works of MM. Gratiolet and Rudolphe Wanger.[2] [p. 342]
And since I have expressed regrets over the lack of precision in the relevant descriptions of lesions of the cerebral hemispheres, I will point out an annoying confusion that has induced error in many observers. Many people, who are in the habit of studying the brain mainly by its inferior face, imagine that the anterior lobes include only the part of the hemispheres that is situated in front of the chiasm of the optic nerves and of the anterior extremity of the temporal-sphenoidal lobe. This is almost, in effect, like stopping at the inferior face of the anterior lobes; but, looking at the convex sides of the hemispheres, these lobes have a length at least double that above, and extend below the fissure of Sylvius, of which they form the superior edge, up to the sulcus of Rolando, which separates them from the parietal lobes. When one reads, in certain observations, that ill people who have had the two anterior lobes entirely destroyed continued to speak up to the moment of their death, it is permitted to believe, in the absence of any other indication, that the author wanted to speak mainly of the lobes that cover the orbital arch. It is said, for example, in the most celebrated of these observations, that a man, injured in the forehead by a mine explosion, had his two anterior lobes entirely crushed and reduced to pulp. But it is clear that no traumatic action can pound immediately, completely and in the same blow the totality of the two anterior lobes without crushing at the same time the whole front half of the brain, including the insula, the striate body, the corpus callosum, the arch to three pillars, etc., and this kind of lesion is not admissible in a man who had been able to walk to his bed, who had retained all his intelligence, and who had survived twenty-four hours without having presented either contracture or paralysis. Similarly, when I exhibited for the first time, at a meeting of physicians, the brain of the man of which I today publish my observations, many people cried out that this work was in contradiction with the ideas of Mr. Bouillaud, that the anterior lobes were very nearly healthy, that the lesion was almost entirely behind these lobes. One will see nevertheless that the frontal (or anterior) convolutions were destroyed to a very considerable extent.
But I have to excuse myself for having developed too far [p. 343] these preliminary remarks. It is time to pass to the relation of my observation of aphemia.
II.
Aphemia dating to twenty-one years, produced by the chronic and progressive softening
of the second and third convolutions of the upper level of the left frontal lobe.
On 11 April 1861, transported to the general infirmary of Bicêtre, surgery service, was a 50-year-old man, named Leborgne, suffering from a diffuse, gangrenous phlegmon of the entire right inferior limb, from the instep up to the buttock. To the questions that I addressed to him the next day on the origin of his malady, he responded only with the monosyllable tan, repeated two times in sequence, and accompanied by a gesture of his left hand. I went for information on this man's history, who had been at Bicêtre for twenty-one years. I interrogated in turn his minders (surveillants), his fellows on the ward, and his parents, who came to see him, and here is what resulted from this inquest.
He was subject, since his youth, to attacks of epilepsy; but he had been able to take up the trade of a hat-form maker [prendre l'état de formier] that he exercised up to the age of thirty. At this time, he lost the ability to speak, and it was for this reason that he was admitted as a patient to the hospice of Bicêtre. We did not know if the loss of speech came on slowly or rapidly, nor if any other symptoms had accompanied the onset of this affliction.
When he arrived at Bicêtre, it had already been two or three months that he had not been able to speak. He was then perfectly healthy and intelligent, and differed from a sane man only in the loss of articulated speech. He came and went in the hospice where he was known under the name of Tan. He understood all that was said to him; he even had very fine hearing; but, regardless of the question addressed to him, he always responded: tan, tan, in conjunction with greatly varied gestures by means of which he succeeded in expressing most of his ideas. When his interlocutors did not comprehend his mime, he would easily become enraged, and then add to his [p. 344] vocabulary a great swearword, one only, and precisely the same that I indicated above, in speaking of a patient observed by Mr. Auburtin. Tan was regarded as being egotistical, vindictive, bad, and his comrades, who detested him, accused him even of being a thief. These faults could have been due in large part to the cerebral lesion; however, they were not pronounced enough to appear pathological, and, though this patient was at Bicêtre, one never thought of moving him to the division for the insane. He was considered, on the contrary, as a man perfectly responsible for his acts.
He had already been without speech for ten years when a new symptom appeared: the muscles of his right arm gradually weakened, and finally became entirely paralyzed. Tan continued to walk without difficulty, but the paralysis of movement won little by little the right inferior limb, and, after having dragged his leg for some time, the patient had to resign himself to keeping constantly to bed. It was about four years from the start of the paralysis of his arm up to the moment when that of his abdominal limb was advanced enough to render standing completely impossible. It was, therefore, close to seven years that Tan was in bed before he was brought to the infirmary. This last period of his life is that of which we have the least information. Having become incapable of doing harm, his comrades no longer occupied themselves with him, except for amusing themselves at his expense a few times (which gave him bitter fits of anger), and he had lost the little celebrity that the singularity of his illness had formerly given him in the hospice. It was noticed that his vision had declined notably over about the previous two years. This was the only complication noticed while he had been confined to his bed. Besides that, he had never been senile; his clothes were changed only once per week, with the result that the widespread phlegmon, for which he was transported to the infirmary on 11 April 1861, was recognized by the nurses only when it had progressed considerably and had invaded the totality of his right abdominal limb, from the foot to the buttock.
The study of this unfortunate person, who could not speak and who, being paralyzed in the right hand, could not write, presented quite a few difficulties. He was moreover in such a generally grave state, [p. 345] that it would have been cruel to torment him with lengthy investigations.
I noted however that his general sensitivity was everywhere preserved, though it was uneven. The right half of his body was less sensitive than the other, and this doubtless contributed to the attenuation of the pain of the extensive phlegmon. The patient did not suffer much when not touched there, but palpation was painful, and a few incisions, that I was obliged to make, provoked agitation and cries.
The two right limbs were completely paralyzed of movement; the two other limbs were obedient to will, and, though weak, could, without any hesitation, execute all movements. The emission of urine and fecal matter was natural, but swallowing was done with some difficulty; mastication, on the contrary, was done very well. The face was not distorted; however, in the act of breathing, the left cheek seemed a little more swollen than the right, thus indicating that the muscles on this side of the face were a little weakened. There was no indication of strabismus. The tongue was perfectly free; it was not distorted; the patient could move it in all directions and stick it out of his mouth. The two halves of this organ were of equal thickness. The difficulty in swallowing that I mentioned above was due to a paralysis starting in the pharynx, and not to a paralysis of the tongue, for it was only the third time swallowing that was laborious. The muscles of the larynx seemed in no way altered, the quality of the voice was natural, and the sounds that the patient made in pronouncing his monosyllable were perfectly clear.
His hearing had kept it fineness: Tan heard well the tick of a watch; but his vision was weak; when he wanted to see the time, he was obliged to take the watch himself with his left hand and place it in a particular position, about 20 centimeters from his right eye, which seemed better than the left.
The state of intelligence could not be exactly determined. It is certain that Tan understood almost everything that was said to him; but, he could only express his ideas or his desires by the movement of his left hand, our dying person [moribond] could not make himself [p. 346] understood as well as he could understand others. Numerical responses were those that he could make the best, by opening or closing his fingers. I asked him many times how many days he had been sick? he [sic] responded sometimes five days, sometimes six days. For how many years had he been at Bicêtre? he [sic] opened his hand four times in sequence, and then pointed with a single finger; this would make twenty-one years, and one saw above that this information was perfectly exact. The next day, I repeated the same question, and I obtained the same response; but, when I wanted to return to this a third time, Tan understood that I was making him do an exercise; he became angry, and articulated the curse already named which I only heard from his mouth one time. I presented him with my watch two days in a row. The second hand was not moving; he could not, as a result, distinguish the three hands other than by their form or by their length; nevertheless, after having examined the watch for a few moments, he was able each time to indicate the time with exactitude. It is therefore incontestable that this man was intelligent, that he could reflect, and that he had preserved, in a certain measure, his memory for things past. He could even comprehend relatively complicated ideas: for instance, I asked him in what order his paralysis had progressed; he made first with the index finger of his left hand a little horizontal gesture that wanted to say: understand! then he pointed successively to his tongue, his right arm and his right leg. It was perfectly exact, apart from the fact that he attributed his loss of speech to paralysis of his tongue, which was very natural.
Nevertheless, various questions to which a man of ordinary intelligence would have found the means to respond to by gesture, even with a single hand, remained without response. Other times, one could not grasp the meaning of certain responses, which seemed to greatly annoy the patient; other times, at last, the response was clear, but false: thus, although he did not have children, he claimed to have them. It is not therefore doubtful that the intelligence of this man had undergone a profound change, being under the influence of his cerebral affliction, being under the influence of the fever that devoured him; but he was evidently much more intelligent than he had to be in order to speak.
It was seen clearly in the information obtained and in the present [p. 347] state of the patient that there existed a progressive cerebral lesion that, originally and during the first ten years of the sickness, was kept limited to a relatively circumscribed region, and which, in this first period, affected neither the organs of motility, nor the organs of sensitivity; that at the end of ten years, the lesion propagated to one or many organs of motility, but not yet [en respectant encore] the organs of sensitivity; and that, more recently finally, general sensitivity was blunted at the same time as vision, especially the vision of the left eye. With the complete paralysis of movement in the two limbs on the right side, and the sensitivity of these two limbs being moreover a little weak, the principle cerebral lesion had to occupy the left hemisphere, and what confirmed this opinion was the incomplete paralysis of the muscles of the left cheek and the retina of the same side, for it need not be repeated [inutile de rappeler] that paralyses of cerebral causes are crossed for the trunk and the limbs, and direct for the face.
It was a matter of determining more exactly, if possible, the seat of the original lesion, and, though the last discussion of the Anthropological Society left some doubt about the doctrine of Mr. Bouillaud, I wanted, in the upcoming autopsy, to proceed as if this doctrine were true; this was the best means of putting it to the test. Mr. Aubertin, having declared some days before that he would renounce it if one could show him a single case of aphemia, well-described, without a lesion to the anterior lobes, I invited him to come see my patient in order to know ahead of time what his diagnosis would be, and if this case was one of those in which he would accept the result as conclusive. Apart from the complications that had been observed for 11 years, my colleague found the current state and the antecedents sufficiently clear to affirm without hesitation that the lesion must have started in one of the anterior lobes.
Reasoning from this datum to complete the diagnosis, I considered that the striate body was the motor organ closest to the anterior lobes; it was without doubt in gradually spreading to this organ that the original lesion had produced the hemiplegia. The probable diagnosis was therefore: original lesion in the left anterior lobe, propagated to the striate body of the same side. As for the nature of this lesion, everything indicated that it was a matter [p. 348] of a progressive, chronic softening, but extremely slow, for the absence of all phenomena of compression excluded the idea of an intracranial tumor.
The patient died on 17 April, at eleven o'clock in the morning. The autopsy was done as soon as possible, that is to say, at the end of twenty-four hours. The temperature was slightly elevated. The cadaver showed no sign of putrefaction. The brain was shown a few hours later to the Anthropological Society, then placed immediately in alcohol. The organ was so altered that we had to take great precautions to conserve it. It was only after two months and after many changes of liquid that the specimen [pièce] began to firm up. Today it is in prefect condition, and it is deposited in the Dupuytren museum under no. 55a, of the nervous system.
I will not relate [passe sous silence] the details relevant to the diffuse phlegmon. The muscles of the two right limbs were entirely fatty and reduced to a small volume. All the viscera were healthy, except the brain.
The skull was opened with a saw with a great deal of care. All the sutures were knit together; the thickness of bone was a little increased; the diploe was replaced by compact tissue. The internal surface of the cranial vault presented in all its extent an appearance of fine wormholes [vermoulure], a certain indication of chronic osteitis (no. 55b).
The external face of the dura mater was red or very vascularized; the membrane was very thick, very vascularized, almost fleshy, and internally covered with a pseudo-membranous film infiltrated with serous fluid, and the appearance of grease [lardacée]. The dura mater and the false membrane together had an average thickness of 5 millimeters (minimum, 3 millimeters; maximum, 8); from which it necessarily follows that the brain must have lost a notable portion of its original volume.
Lifting the dura mater, the pia mater appeared very perforated [injectée] at certain points, thick throughout, and, in places, opaque, infiltrated with a plastic yellowish material that had the color of puss, but that was solid, and that, when examined through a microscope, did not contain purulent globules.
On the lateral part of the left hemisphere, at the level of the Sylvian fissure, the pia mater was raised by an amount of [p. 349] transparent serous fluid, that was lodged in a large and deep depression of the cerebral substance. This liquid was evacuated by puncturing it, collapsing the pia mater, pushing it down deeply, and resulting in the opening of a long cavity of capacity equivalent to the volume of a chicken egg, connected to the Sylvian fissure, and separating thereby the frontal lobe from the temporal lobe. It extended at the rear up to the level of the sulcus of Rolando, which separates, as we know, the anterior or frontal convolutions from the parietal convolutions. The lesion was therefore situated throughout the entire region in front of this sulcus, and the parietal lobe was healthy, at least relatively speaking [d'une manière relative], for no part of the hemispheres was in a state of absolute integrity.
In cutting and peeling back [écartant] the pia mater at the level of the cavity I have here described, one recognized at first glance that this corresponded not to a depression, but to a loss of substance of the cerebral mass; the liquid that filled it had been produced continuously to fill the space as it formed, as took the place of the chronic softening of the superficial layers of the brain or the cerebellum [cervelet]. The study of the convolutions that formed the edges of the cavity effectively demonstrates that they were the seat of one of these chronic softenings of which the progress was slow enough that the cerebral molecules, dissociated in some way one from another, were able to be absorbed [résorber] and be replaced by an emission of serous fluid.[3] A notable part of the left hemisphere had thus been destroyed gradually; but the softening extended well beyond the limits of the cavity; this was by no means circumscribed, and cannot under any circumstances be described as a cyst. Its inner faces [parois], irregular and with crevices almost everywhere, were constituted of the cerebral substance itself, which was extremely soft at this level, and which the most internal surface, in direct [p. 350] contact with the secreted serous fluid, was on its way to slow and gradual dissolution when the patient succumbed. The inferior face alone was smooth and had a quite firm consistency.
It is clear, consequently, that the original home of the softening was where today is found the loss of substance, that the illness thereafter expanded to further and further through the continuity of tissue, and that the point where it started is to be found not within the organs now softened, or on their way to softening, but among those which are more or less completely destroyed. We will therefore, based on inspection of the parts that limit the loss of substance, draw up the list of those that have disappeared.
The cavity that we will described is situated, as we have already seen, at the level of the Sylvian fissure; it consequently lies between the frontal lobe and the temporal-sphenoïdal lobe, and if the organs that surround it were only interfered with [refoulés] without being destroyed, one should find on its inferior or temporal side the marginal inferior convolution, on its superior or frontal side the third frontal convolution[4], and finally, on its inner face, [p. 351] the lobe of the insula. Now, this is not without significance [il n'en est rien]. 1) The inferior face of the cavity is limited by the second temporo-sphenoïdal [p. 352] convolution, which was moreover entirely intact, and which possessed a quite firm consistency. The entire thickness of the marginal inferior convolution had therefore been destroyed, that is to say, up to the parallel fissure. 2) The deep wall of the cavity no longer presents traces of the lobe of the insula; this lobe is entirely destroyed, as well as the inner half of the extra-ventricular nucleus of the striate body; finally, the loss of substance is extended from this side up to the anterior part of the ventricular nucleus of the striate body, of such a sort that our cavity connects [communique], by a long opening of half a centimeter and with irregular edges, with the lateral ventricle of the brain. 3) Finally, the superior edge, or rather, the superior wall of the cavity, encroaches considerably on the frontal lobe, which presents at this level a large and deep indentation. The posterior half of the third frontal convolution is completely destroyed throughout all its thickness; the second frontal convolution is a little less altered. At least its two external layers have disappeared, and the external layer, which is still in place [retrouve], is extremely softened. Behind, the inferior layer of the frontal transversal convolution is destroyed, throughout its thickness, up to the Rolandic sulcus.
In summary, as a consequence, the destroyed organs are the following:
The small inferior marginal convolution (temporo-sphenoïdal lobe); the small convolutions of the lobe of the insula, and the part subjacent to the striate body; finally, on the frontal lobe, the inferior part of the transversal convolution, and the posterior half of the two great convolutions designated by the name of second and third frontal convolutions. Of the four convolutions that form the superior layer of the frontal lobe, one alone, the first and the most internal, did not preserve its integrity, for it is softened and atrophied, but did preserve its continuity; and if one imaginatively restores [rétablit par la pensée] all the parts that have been destroyed, one finds that at least three-quarters of the cavity that has been hollowed out comes from the frontal lobe.
It now remains to be determined the location at which the lesion must have begun. Now, examination of the cavity left by the loss of substance shows first of all that the center of its focus [foyer] corresponds to the frontal lobe. As a consequence, if the softening had spread [p. 353] uniformly in all directions, this lobe would have been the point of departure for the illness. But it is not only the study of the cavity that should guide us, we should also take account of the state of the parts that surround it. These parts are very unequally softened, they are affected to a highly variable extent. Thus, the second temporal convolution, that forms the inferior limit of the focus, presents a smooth surface and relatively firm consistency; it is softened, without doubt, but is not much so, and it is softened only in its uppermost layer. On the opposing side, on the frontal lobe, the softening is, by contrast, almost fluid in the neighborhood of the focus; as one increases one's distance from it, the cerebral substance gradually becomes firmer, but the softening extends, in reality, up to a considerable distance, and reaches almost all of the frontal lobe. It is therefore primarily in this lobe that the softening was propagated, and it is almost certain that the other parts were invaded subsequently.
If one were looking to be more precise, one might remark that the third frontal convolution is that which presents the most extensive loss of substance, that it is not only cut across the level of the anterior extremity of the Sylvian fissure, but still is entirely destroyed throughout its posterior half, that it alone has suffered a loss of substance equal to about half of the total loss of substance; that the second convolution, or middle convolution, although very profoundly damaged, still preserves the continuity of its most internal part, and that as a consequence, according to all probabilities, it is in the third frontal convolution that the disease began.
The other parts of the hemispheres are relatively healthy; they are, it is true, a little less firm than is typical, and one can say that all the exterior parts of the encephalon have suffered notable atrophy, but they have preserved their form, their continuity, their normal aspect. As for the deep parts, I abstained [renoncé] from studying them, so as not to destroy the specimen, which it seemed important to me to deposit in the Museum. However, the opening that connects the exterior to the anterior part of the left lateral ventricle was, despite my efforts, enlarged during the dissection of the pia mater so that I was able to examine half the internal surface of this ventricle, and I saw that all of the striate body was [p. 354] more or less softened, but that the optic stratum maintained [avait] its color, its volume, and its normal consistency.
The whole encephalon, weighed with the pia mater, after evacuation of the liquid that filled the focus, was not greater than 987 grams. It is therefore almost 400 grams lighter than the average weight of the brains of 50-year-old men. This considerable loss was carried almost entirely by the cerebral hemispheres. One knows, in effect, that the rest of the encephalon in a normal state, never reaches the weight of 200 grams, and stays almost constantly below 180. Now, the cerebellum, the protuberance and the bulb, although not voluminous in our subject, are certainly not much below the average, and in supposing, impossibly, that they had lost a quarter of their weight, this would account only for a minimal part of the total loss.
The destruction of the organs that surround the Sylvian fissure of the left hemisphere contributes, no doubt, much to the diminution of the brain weight; but I have taken from a healthy brain the same amount of substance, and the mass that I lifted weighed no more than 50 grams. It is therefore infinitely probable that the cerebral hemispheres have suffered, throughout their extent, a quite considerable atrophy, and this probability is changed to certitude if one considers the relative thickness of the meninges and of the distorted [fausse] arachnoid membrane, that reaches a thickness at certain points of 5 or 6 millimeters.
After having described these lesions, and researched their nature, seat, and anatomical progression, it is important to compare these results with those of clinical observation, to finally establish, if possible, a connection between the symptoms and the material disorders.
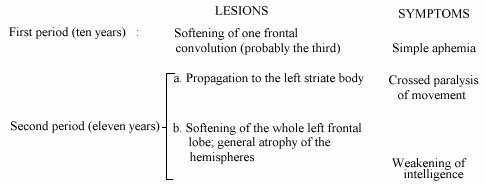
Anatomical inspection shows that the lesion was still in the act of propagating when the patient succumbed. The lesion had therefore been progressive, but it advanced very slowly, since it had taken twenty-one years to destroy a quite limited part of the cerebral mass. It is permissible to believe, as a consequence, that there was a long period during which it did not go beyond the limits of the organ in which it had started. Now, we saw that the original focus of the illness was situated in [p. 355] the frontal lobe, and quite probably in the third frontal convolution. This drives us to admit that from the point of view of pathological anatomy there had been two periods: one in which only one frontal convolution (probably the third) was altered; the other, in which the illness propagated itself little by little to the other convolutions, to the lobe of the insula or to the extra-ventricular nucleus of the striate body.
If now we examine the succession of symptoms, we find equally two periods: a first period which lasted ten years, during which the faculty of language was abolished, and when all the other functions of the encephalon were intact; and a second period of eleven years, during which a paralysis of movement, at first partial, then absolutely complete, successively invaded the superior limb and the inferior limb of the right side.
Having said this, it is impossible [not] to recognize that there had been a correspondence between the two anatomical periods and the two symptomological periods. Nor to ignore that the cerebral convolutions are not motor organs. The striate body of the left hemisphere is therefore of all the organs damaged [léssé] the only one in which one can find the cause of the paralysis of the two right limbs, and the second clinical period, that in which motility was altered, corresponds also to the second anatomical period, that is to say, to that in which the softening, overflowing the limits of the frontal lobe, reached the insula and the striate body.
Thus, the first period of ten years, characterized clinically by the unique symptom of aphemia, must correspond to the phase [époque] in which in the lesion was still limited to the frontal lobe.
Up to now, given the parallel between lesions and symptoms, I have mentioned neither troubles of intelligence, nor of their anatomical cause. We have seen that the intelligence of our patient, perfectly preserved for a long time, declined notably beginning at a time [époque] that cannot be determined, and that it was seriously weakened when we observed it for the first time. We found, in the autopsy, alterations more than sufficient to explain this state. Three frontal convolutions of four were profoundly damaged to a considerable extent, nearly the whole frontal lobe was more or less softened; finally all the mass [p. 356] of the convolutions of the two hemispheres were atrophied, sunken, and sensibly softer than in the normal state. One can scarcely understand that the patient was able to retain any intelligence at all, and it does not seem probable that one could live very long with this kind of brain. I think, for my part, that the general softening of the left frontal lobe, the general atrophy of the two hemispheres, and the general chronic meningitis, did not appear at a time much in the past [ne remontaient pas à une époque fort reculée]; I am disposed to believe that these lesions came about a long time after the softening of the striate body, of the sort that one could subdivide the second period into two secondary periods, and in doing so, summarize the history of the patient.
Facts that, like these ones, are attached to grand questions of doctrine, cannot be presented in too much detail, nor discussed with too much care. I need this excuse to pardon myself for the aridity of the description and the length of the discussion. I now only have but a few more words to add to bring out the consequences of this study.
1st Aphemia, that is to say the loss of speech, before all other intellectual trouble and before all paralysis, was the consequence of a lesion of one of the anterior lobes of the brain.
2nd Our observations therefore confirm the opinion of Mr. Bouillaud, who places in these lobes the seat of the faculty of articulated language.
3rd The observations assembled up to now, those at least that are accompanied by a clear and precise anatomical description, are not numerous enough that one can consider this localization of a particular faculty in a lobe to be determined [p. 357] like a definitive demonstration, but one can consider it at least extremely probable.
4th It is a much more difficult question to know whether the faculty of articulated language depends on the anterior lobe considered as a whole, or especially on one of the convolutions of this lobe; to know, in other terms, if the localization of the cerebral faculties is arranged one faculty per convolution, or only by groups of faculties and groups of convolutions. More observations should be collected with the goal of resolving this question. We must indicate exactly the name and the row of the ill convolutions, and, if the lesion is very extensive, to determine, as far as possible, by anatomical examination, the point in the convolution where the illness seems to have started.
5th In our patient, the original seat of the lesion was in the second or the third frontal convolution, more probably in the latter. It is therefore possible that the faculty of articulated language resides in one or the other of these two convolutions; but one still cannot know, considering that the previous observations are mute on the state of each convolution in particular, and one cannot even predict, since the principle of localization by convolution still rests on no certain basis.
6th In any case, it suffices to compare our observations with those that have preceded them to dismiss today the idea that the faculty of articulated language resides at a fixed point, circumscribed, and situated under any bump of the skull; the lesions of aphemia have been found most often in the most anterior part of the frontal lobe, not far from the eyebrow, and above the orbital arch; whereas in my patient, they exist mostly in front, and much more near the coronal suture than near the sourciliary arcade. This difference of seats is incompatible with the system of bumps; it would be perfectly coincident, by contrast, with the system of localizations by convolution, since each of the three great convolutions of the superior layer of the frontal lobe travel successively, in its antero-posterior trajectory, to all the regions in which have been found up to now the lesions of aphemia.
Footnotes
[1] It is generally believed that the sulcus of Rolando is situated directly beneath the coronal suture, and Mr. Gratiolet, following this, accords very particular importance to the study of this suture, which would permit the establishment of a very precise relation between the frontal region of the skull and the anterior lobes of the brain. This would be an infinitely precious datum [donnée] in the comparison of the human races. Unfortunately, this datum is completely inaccurate: the brain, taken out of the skull and placed on a table, is slack [s'étale] and stretched, and if one measures the length of the anterior lobe of the hemisphere, one finds that it is nearly equal to that of the frontal bone. But, in examining the organs in place, I have arrived at a completely different result. Here is how I proceed. After having lifted the integument and the pericranium, I sink gimlets [vrilles] at various points of the coronal suture, and I push through the gimlet holes little wooden pins [chevilles] into the cerebral substance. The skull is then opened with a saw; the brain is lifted and stripped of its membranes, and I study the situation of the pins with respect to [par rapport au] the sulcus of Rolando. I have done this research on eleven subjects of the masculine sex, having reached or surpassed the age of adulthood, and I have found consistently that the sulcus of Rolando begins, on the median line, at least 4 centimeters behind the coronal suture, (minimum 40 millimeters; maximum 63 millimeters). At its external part, this sulcus, which is oblique and not transverse, is brought together with the coronal suture; at 4 centimeters from the median line, it is situated only 2 centimeters at least, 3 at most, behind this suture. The same procedure has permitted me to verify that there is to the contrary a quite constant relation between the lambdoid suture and the occipital transverse sulcus that separates the parietal lobe from the occipital lobe of the hemisphere. The pins sunk into the lambdoid suture ordinarily penetrate the occipital sulcus or very near to it. I have never found them more than 15 millimeters from this sulcus, and the deviation [écart] is rarely more than 5 millimeters.
[2] Gratiolet et Leuret, Anatomie comparée du système nerveux, 1. II, p. 110, Paris, 1857, in-8. The second volume is exclusively the work of Mr. Gratiolet. -- Gratiolet, Mémoire sur les plis cérébraux de l'homme et des primates, Paris, 1854, in-4, with atlas in-folio. -- Rudolphe Wagner, Abhandlung über die typischen Verschiedenheiten der Windungen der Hemisphæren, etc., Gottingen, 1860, in-4, with atlas, p. 13 to 25. One will find further on, in another note, an abridged description of the anterior or frontal convolutions.
[3] It is thus not that these things happened in the softening that started in the medullary layer of the convolutions: it is only when the lesion has its point of departure under the pia mater, that is in the cortical layer of the convolutions, that the softened and slowly-absorbed substance is replaced by the serous fluid. I observed the diverse phases of this mechanism on the cerebellum as well as the on the cerebrum [cerveau]. The first work [pièce] that I reported [recueillie] (and that I presented in January 1861 to the Anatomical Society) first confused me; but since then many others have relieved [levé] my doubts.
[4] It seemed to me necessary, for understanding that which follows, to recall here, in summary form, the disposition of and relations among the cerebral organs that I should mention.
The anterior lobe of the brain includes the whole part of the hemisphere situated above the Sylvian fissure, which separates it from the temporo-sphenoïdal lobe, and in front of the Rolandic sulcus, which separates it from the parietal lobe. The location of the latter sulcus has been made precise in a previous note (p. 340). Its direction is nearly transverse; starting at the median line, it goes almost in a straight line, having hardly any bends, to end at its lower and outside point at [décrivant à peine de légères flexuosités, aboutir en bas et en dehors à] the Sylvian fissure, which it meets almost at a right angle, behind the posterior edge of the lobe of the insula.
The anterior lobe of the brain is composed of two layers, the inferior or orbital one, formed of many convolutions known as orbital, that lie on the vault [vôute] of the orbit, and of which I will have nothing to say; the other superior, located under the shell [écaille] of the frontal bone and under the most forward part of the parietal.
This superior layer is composed of four fundamental convolutions, that are known as the frontal convolutions, properly called: one is posterior, the others are anterior. The posterior, not very flexuous [peu flexeuse], forms the anterior edge of the Rolandic sulcus; it is therefore almost transversal, and it turns back from outside to inside, from the Sylvian fissure to the great median fissure that receives the falx of the brain: this is why one designates it indifferently by the names of frontal posterior convolution, transversal or ascendant. The three other convolutions of the superior layer are very flexuous, very complicated, and one must have a certain knack [habitude] for distinguishing them along their full length, in order to avoid confusing the fundamental sulci that separate them, with the secondary sulci that separate the second-order layers, and that vary, following the individual ones, according to the degree of complication, that is to say according to the degree of development of the fundamental convolutions. These three anterior convolutions are antero-posterior, and, run side by side, covering from front to back the full length of the frontal lobe. They start at the level of the sourciliary arcade, from which they bend back and continue [se réfléchissent pour se continuer] along the convolutions of the inferior layer, and end, in the back, at the frontal transversal convolution, into which all three empty. They carry the names of first, second, and third frontal convolutions. One can also call them internal, middle [moyenne], and external; but the ordinary terms are more prevalent.
The first goes along with the great fissure of the brain; it consistently presents, in the human species, a more or less complete antero-posterior sulcus that divides into two folds of the second-order. It is therefore divided into two convolutions; but the comparative anatomy shows that these two folds form only a single fundamental convolution.
The second frontal convolution offers nothing in particular; it is not the same as the third, which is the most external. This one presents a superior or internal edge contiguous with the fluxuous edge of the middle convolution, and an inferior or external edge the connections [rapports] of which differ depending on whether one examines them at the front or back. In its anterior half, this edge is in contact with the external edge of the most external orbital convolution. In its posterior half, it is free, by contrast, and separated from the temporo-sphenoïdal lobe by the Sylvian fissure, of which it forms the superior edge. It is because of this last connection that the third frontal convolution is sometimes designated by the name of marginal superior convolution.
We add that the inferior edge of the Sylvian fissure is formed by the superior convolution of the temporo-sphenoïdal lobe, which is for this reason called the marginal inferior convolution. It is an antero-posterior fold, thin and almost rectilinear, which is separated from the second temporo-sphenoïdal convolution by a sulcus parallel to the Sylvian fissure. This sulcus is designated by the name of parallel fissure (insinuated into the Sylvian fissure).
Finally, when one spreads apart the two marginal convolutions, superior and inferior, of the Sylvian fissure, one perceives a large hill [éminence] and a small bulge [saillante] the summit of which gives birth to five small simple convolutions, or rather to five rectilinear folds radiating in the shape of a fan: this is the lobe of the insula which covers the extra-ventricular nucleus [noyau] of the striate body, and which, rising from the base of the Sylvian fissure, is found to be a continuous substance, via its cortical layer, with the deepest part of the two marginal convolutions, by its medullary layer with the extra-ventricular nucleus of the striate body. It follows from this connection that a lesion that is spread, by way of this continuity, from the frontal lobe to the temporo-sphenoïdal lobe, or reciprocally, passes almost necessarily by the lobe of the insula, and that from there it is likely to spread to the extra-ventricular nucleus of the striate body, given [attendu] that the substance of the insula proper, which separates this nucleus from the surface of the brain, forms only a very thin layer.